A T-cell positive, B-cell negative allo flow crossmatch with a double-negative auto flow crossmatch: Interference of therapeutic brodalumab in a kidney transplant patient with psoriasis
(P708) A T-cell positive, B-cell negative allo flow crossmatch with a double-negative auto flow crossmatch
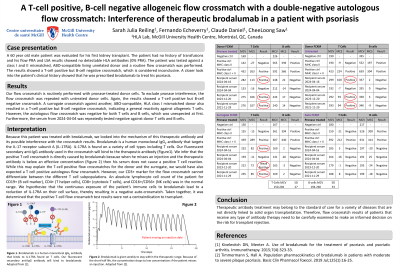
Body: A 60 year old male patient was evaluated for his first kidney transplant. The patient had no history of transfusions and his flow PRA and LSA results showed no detectable HLA antibodies (0% PRA). The patient was matched with an ABO-compatible donor and a routine flow crossmatch was performed. The results showed a T-cell positive but B-cell negative crossmatch, which is considered inconclusive. A repeat flow crossmatch with unpronased donor cells was also T-cell positive but B-cell negative. A surrogate crossmatch against another HLA class I mismatched donor was, again, T-cell positive but B-cell negative, indicating a general reactivity against allo T cells. However, the auto flow crossmatch was negative for both T cells and B cells, which was unexpected at first. A closer look into the patient’s clinical history showed that he was prescribed brodalumab to treat his psoriasis. Brodalumab is a human monoclonal IgG2 antibody that targets the IL-17 receptor subunit A (IL-17RA). IL-17RA is found on a variety of cell types including T cells. We infer that the positive T cell crossmatch is directly caused by brodalumab because when he misses an injection his serum does not cause a positive T cell reaction. While this may explain the T-cell positive flow crossmatches for the donor and the surrogate, we would have also expected a T-cell positive auto flow crossmatch. However, our CD3+ marker for the flow crossmatch cannot differentiate between the different T cell subpopulations. An absolute lymphocyte cell count of the patient for CD19+ (B cell marker), CD4+ (T helper cells), CD8+ (cytotoxic T cells), and CD16+/CD56+ (NK cells) was in the normal range. We hypothesize that the continuous exposure of the patient’s immune cells to brodalumab lead to a reduction of IL-17RA on their cell surface, thereby resulting in a negative crossmatch. Taken together, it was determined that the flow crossmatch test results were not a contraindication to transplant.
Conclusion: Therapeutic antibody treatment may belong to the standard of care for a variety of diseases that are not directly linked to solid organ transplantation. Therefore, flow crossmatch results of patients that receive any type of antibody therapy need to be carefully examined to make an informed decision on the risk for transplant rejection.