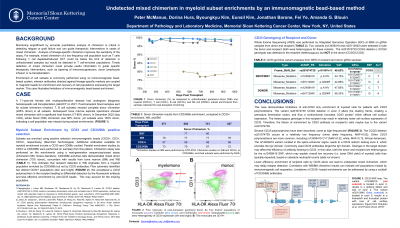
Body: Monitoring engraftment by chimerism status is critical in detecting relapse or graft failure and can guide therapeutic interventions in cases of mixed chimerism. Analysis of subset enrichments improves the sensitivity of the assay. This case illustrates limitations of immunomagnetic bead-based enrichment. A 71-year-old female with myeloproliferative disease had undergone allogeneic hematopoietic cell transplant (alloHCT) in 2021. Post-transplant blood samples sent for subset chimerism (myeloid, T, B cell subsets) showed complete donor chimerism (≥95% donor) in all subsets. In December 2022 (day +545), whole blood (WB) chimerism was 80% donor, yet subsets were 100% donor, indicating a cell population was missed during subset enrichments. (FIGURE 1). Subsets are enriched using positive selection immunomagnetic beads (CD33+, CD3+, CD19+, respectively) (StemCell Technologies). Additional antibodies available for myeloid enrichment include a CD33 and CD66b cocktail. Parallel enrichment studies by CD33 vs CD33/66b were performed on samples from this patient. Chimerism assay was performed on the enrichments using a next-generation sequencing-based assay (Chimerism MD, Scisco-Genetics). CD33/66b enriched cells demonstrated mixed donor chimerism (73% donor), concordant with results from bone marrow (BM) and WB (TABLE 1). This indicates that recipient detected in WB originates from a myeloid population enriched by CD33/66b but not by CD33 antibodies. Flow cytometry identified two distinct CD33+ populations (dim and bright). We considered a CD33 polymorphism in the recipient leading to differential detection by the fluorescent antibody and less effective enrichment by anti-CD33 beads. This may account for the missing population. CD33 genotyping of recipient and donor is pending.
Conclusion: This case demonstrates limitations of anti-CD33 only enrichment of myeloid cells for patients with CD33 polymorphisms. CD33 SNP rs12459419 C>T results in a CD33 isoform lacking exon 2, the IgV domain, a target epitope for many diagnostic and therapeutic anti-CD33 antibodies. Allele frequency for this polymorphism is reported to be highest in Caucasian patients (MAF=0.32). Less efficient enrichment of recipient cells by CD33 alone can lead to undetected mixed chimerism, which may delay relapse detection. Limitation of CD33 based enrichments can be addressed by a cocktail of CD33/66b antibodies.