Aim: Major Histocompatibility complex class I chain-related genes A (MICA) and B (MICB) exhibit polymorphisms that make them important histocompatibility targets. Yet, some populations have not been well characterized. Even less studies have explored MICB allele distribution in populations. We report the MICA and MICB alleles distribution in a US population residing in Georgia and South Carolina. Notably, only one other study has used NGS to type MICA.
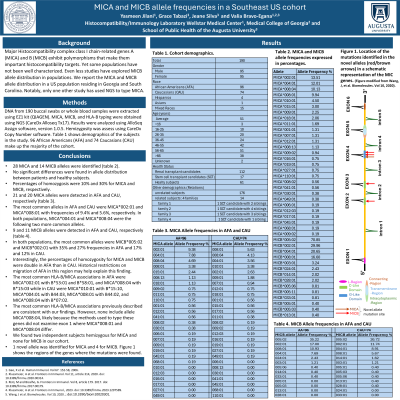
Method: DNA from 190 buccal swabs or whole blood samples was extracted using EZ1 kit. MICA, MICB, and HLA-B typing were obtained using NGS (CareDx Alloseq Tx17). Results were analyzed using AlloSeq Assign software, version 1.0.5. Table 1 shows demographics of the subjects in the study. 96 African Americans (AFA) and 74 Caucasians (CAU) make up the majority of the cohort.
Results: In total, 28 MICA and 14 MICB alleles were identified (table 2). No significant differences were found in allele distribution between patients and healthy subjects. Percentages of homozygosis were 10% and 30% for MICA and MICB, respectively. There were 21 and 20 MICA alleles detected in AFA and CAU, respectively. The most common alleles in AFA and CAU were MICA*002:01 and MICA*008:01 with frequencies of 9.4% and 5.6%, respectively. In both populations, MICA*004:01 and MICA*008:04 were the following 2 more common alleles. For MICB, 9 and 11 alleles were detected in AFA and CAU, respectively. In both populations, the most common alleles were MICB*005:02 and MICB*002:01 with 35% and 27% frequencies in AFA and 17% and 12% in CAU. Interestingly, the percentages of homozygosity for MICA and MICB were double in AFA than in CAU. Historical restrictions on migration of AFA in this region may help explain this finding. The most common HLA-B/MICA associations in AFA were MICA*002:01 with B*53:01 and B*58:01, and MICA*008:04 with B*15:03 while in CAU were MICA*010:01 with B*15:10, MICA*004:01 with B44:03, MICA*008:01 with B44:02, and MICA*008:04 with B*07:02. Most of these associations are consistent with previous studies but they do not include MICA*008:04, likely because the methods used to type these genes did not examine exon 1 where MICA*008:01 and MICA*008:04 differ.
Conclusion: Further studies with a larger number of subjects are necessary to better characterize the distribution of MICA and MICB alleles in different populations and their associations.