Body: A 62-year-old Filipino female who lost her first kidney graft due to chronic allograft nephropathy 21 years post-transplant was listed for evaluation for a second kidney transplant. The patient was withdrawn from immunosuppressants (IS) at the time of relisting; the patient did not receive a nephrectomy. The patient had been at 0% cPRA at the time of transplant and remained so over the life of the graft. The donor was typed as A24, A31, B35 (Bw6), B39 (Bw6), DR4, DR12, DR52, and DR53; -C and -DP antigens were not typed. DQ antigens were deduced using Haplostat Asian Pacific Islander dataset (DQ7 and DQ8). The recipient was typed as homozygous A34, B61 (Bw6), DR15, DR51, and DQ5.
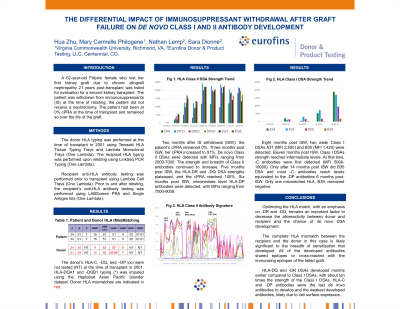
Two months after IS withdrawal (ISW), the patient’s cPRA remained 0%. Three months post ISW, cPRA increased to 91%. De novo Class II DSAs were detected with MFIs ranging from 2000-7000 while Class I DSAs were not detectable. The strength and breadth of Class II antibodies continued to increase (Fig 1). Five months post ISW, the first weak Class I A24 DSA was detected, while the -DR and -DQ DSA strengths plateaued, and the cPRA reached 100% (Figs 1, 2). Six months post ISW, intermediate level DP antibodies were detected, MFIs ranging from 7000-9000. Eight months post ISW, two weak Class I DSAs A31 (MFI 2,500) B35 (MFI 1,420) were detected (Fig 2). Eleven months post ISW, Class I DSAs strength reached intermediate levels. At that time, -C antibodies were first detected (MFI 5000-10000). Only after 14 months post ISW did B35 DSA and most -C antibodies reach levels equivalent to the -DP antibodies 6 months post-ISW. Only one mismatched HLA, B39, remained negative.
Conclusion: Optimizing the HLA match, with an emphasis on -DR and -DQ, remains an important factor to decrease the alloreactivity between donor and recipient. The complete HLA mismatch is likely significant to the breadth of sensitization that developed. All of the developed antibodies shared epitopes or cross-reacted with the immunizing epitopes of the failed graft. -DQ and -DR DSAs developed months earlier compared to Class I DSAs, with about ten times the strength of Class I DSA. -C and -DP antibodies were the last de novo antibodies to develop and weakest developed antibodies, likely due to cell surface expression.