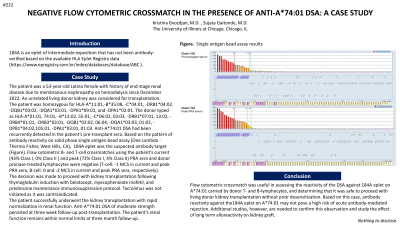
Body: 184A is an eplet of intermediate exposition that has not been antibody-verified based on the available HLA Eplet Registry data (https://www.epregistry.com.br/index/databases/database/ABC ). The patient was a 53-year-old Latino female with history of end-stage renal disease due to membranous nephropathy on hemodialysis since December 2022. An unrelated living donor kidney was considered for transplantation. The patient was homozygous for HLA-A*11:01,-B*35:08, -C*04:01, -DRB1*04:02, -DQB1*03:02, -DQA1*03:01, -DPB1*09:01, and -DPA1*02:01. The donor typed as HLA-A*01:01, 74:01, -B*13:02, 55:01, -C*06:02, 03:03, -DRB1*07:01, 13:02, -DRB4*01:01, -DRB3*03:01, -DQB1*02:02, 06:04, -DQA1*03:03, 01:02, -DPB1*04:02, 105:01, -DPA1*03:01, 01:03. Anti-A*74:01 DSA had been recurrently detected in the patient’s pre-transplant sera. Based on the pattern of antibody reactivity on solid phase single antigen bead assay (One Lambda - Thermo Fisher, West Hills, CA), 184A eplet was the suspected antibody target (Figure). Flow cytometric B- and T-cell crossmatches using the patient’s current (43% Class I, 0% Class II ) and peak (72% Class I, 4% Class II) PRA sera and donor pronase-treated lymphocytes were negative (T-cell: -1 MCS in current and peak PRA sera, B-cell: 0 and -2 MCS in current and peak PRA sera, respectively). The decision was made to proceed with kidney transplantation following thymoglobulin induction with belatacept, myecophenolate mofetil, and prednisone maintenance immunosuppression protocol. Tacrolimus was not initiated as it was contraindicated. The patient successfully underwent the kidney transplantation with rapid normalization in renal function. Anti-A*74:01 DSA of moderate strength persisted at three week follow-up post-transplantation. The patient’s renal function remains within normal limits at three month follow-up.
Conclusion: Flow cytometric crossmatch was useful in assessing the reactivity of the DSA against 184A eplet on A*74:01 carried by donor T- and B-lymphocytes, and determining that it was safe to proceed with living donor kidney transplantation without prior desensitization. Based on this case, antibody reactivity against the 184A eplet on A*74:01 may not pose a high risk of acute antibody-mediated rejection. Additional studies, however, are needed to confirm this observation and study the effect of long term alloreactivity on kidney graft.