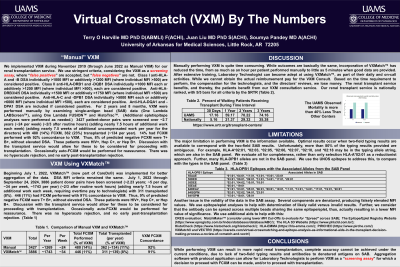
Body: We implemented VXM during November 2019. We used stringent criteria, considering the VXM as a screening assay, where “false positives” are accepted, but “false negatives” are not. Class I anti-HLA-A and -B DSA individually >1000 MFI or additively >1200 MFI (where individual MFI >500) are considered positive. Class II anti-HLA-DRB1 and -DQB1 DSA individually >1000 MFI each or additively >1200 MFI (where individual MFI >500) each are considered positive. Anti-HLA-DRB3/4/5 DSA individually >1500 MFI or additively >1750 MFI (where individual MFI >500) are considered positive. Anti-HLA-C and -DPB1 DSA individually >5000 MFI each or additively >6000 MFI (where individual MFI >500) each are considered positive. Anti-HLA-DQA1 and -DPA1 DSA are included if considered positive. For 2 years and 8 months, VXM were performed manually by examining SAB data (One Lambda LABScreen™), using One Lambda FUSION™ and HistoTrac™. 1554 patient-donor pairs were screened (~11 per week) (~2/3 after routine hours) (adding nearly 7.5 hours of additional work each week) (adding nearly 7.5 weeks of additional uncompensated work per year for the directors) with 362 transplanted (23%) (~136 per year). 29% had FCXM performed with 92% concordance. Thus, 8% of predicted negative FCXM were T+ B+, without elevated DSA.
Beginning July 1, 2022, VXMatch™ (now part of CareDx®) was implemented for better aggregation of the data. Through April 30, 2024, 3289 patient donor pairs have been screened (~1 year 10 months; ~5 per day, ~36 per week, ~1872 per year) (~2/3 after routine work hours) (adding nearly 7.5 hours of additional work each week, requiring overtime pay to technologists) with 248 transplanted (8%). 12% had FCXM performed with 93% concordance. Thus, 7% of predicted negative FCXM were T+ B+, without elevated DSA.
FCXM-positive patients were HIV+, Hep C+, or Hep B+. Discussion with the transplant service would allow for these to be considered for proceeding with transplantation. Occasionally auto-FCXM would be performed. There was no hyperacute rejection, and no early post-transplantation rejection.
Conclusion: Manually performing VXM is quite time-consuming. Incorporation of VXMatch™ has reduced the time. The renal transplant service benefits, and thereby, the patients benefit from our VXM consult service. Our renal transplant service is nationally ranked, with 5/5 bars for all criteria by the SRTR, first in survivability and fourth overall.