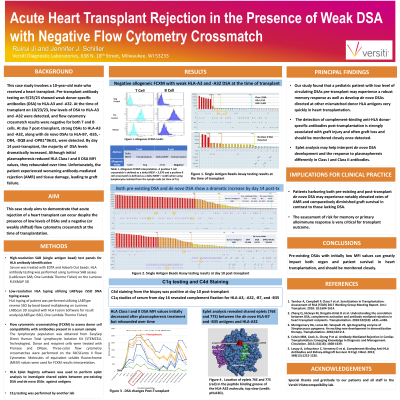
Body: This case study involves a 10-year-old male who received a heart transplant. Pre-transplant antibody testing on a 9/25/23 sample indicated only weak donor-specific antibodies (DSA) to HLA-A3 and -A32, and the clinical team chose to proceed with the organ offer. Single antigen bead testing at the time of transplant on 10/23/23 detected DSA to HLA-A3 (MFI=1,159) and -A32 (MFI=1,401) and Flow Cytometry Crossmatch (FCXM) results were both T cell and B cell negative. In contrast, FCXM with the historic sample were weakly T cell and B cell positive despite having similar DSA MFI values. Post-transplant the patient received blood products and underwent protocol immunosuppression. No Class I antibodies were detected and only a very low level of de novo HLA-DQ8 DSA was detected on day 4 post-transplant. However, by day 7 there were strong DSA to HLA-A3 and -A32 as well as de novo DSAs to HLA-B7, -B35, -DR4, and -DPB1*06:01. By day 10 there was a dramatic increase in DSA to HLA-A3 (MFI=25,303), -A32 (MFI=23,556), -B7 (MFI=21,503), and -B35 (MFI=26,162), along with a moderate increase in DSA to HLA-DR4 (MFI=11,564) and -DPB1*06:01 (MFI=18,824). C4d staining from the biopsy was positive at this time. On day 14 the clinical team initiated plasmapheresis. HLA Class I and II DSA MFI values initially decreased but rebounded over time (Fig. 1). C1q studies of serum from day 16 revealed complement fixation for HLA-A3, -A32, -B7, and -B35. The biopsy conducted on day 24 indicated a worsening in antibody-mediated rejection (AMR) accompanied by tissue damage. Eplet analysis revealed shared eplets (76ES and 77S) between the de novo HLA-B7 and -B35 antigens and HLA-A32, suggesting that de novo DSA development may contribute to stimulation of a memory response and may also help explain why the Class II DSA cleared faster during treatment.
Conclusion: This case highlights the importance of pre-existing DSAs with initially low MFI values, which can greatly impact both organ and patient survival. Individuals with circulating DSAs may experience a robust memory response as well as develop de novo DSAs directed at other mismatched donor HLA antigens very quickly. The detection of complement-binding anti-HLA donor-specific antibodies post-transplantation is strongly associated with graft injury and often graft loss, and should be monitored closely once detected.