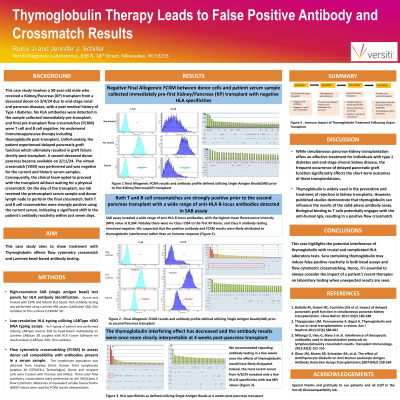
Body: This case study involves a 50-year-old male who developed end-stage renal and pancreas diseases, with a past medical history of Type I diabetes. He received a Kidney/Pancreas (KP) transplant from a deceased donor on 3/4/24. No HLA antibodies were detected in the sample collected immediately pre-transplant, and final pre-transplant flow crossmatches (FCXM) were T cell and B cell negative. He underwent immunosuppressive therapy including thymoglobulin post-transplant. Unfortunately, the patient experienced delayed pancreatic graft function which ultimately resulted in graft failure shortly post-transplant. A 2nd deceased donor pancreas became available on 3/11/24 at which time our lab received the pre-transplant serum and donor lymph nodes for final crossmatching. The results from the Class I single antigen bead (SAB) assay revealed a wide range of anti-HLA B-locus antibodies, with the highest mean fluorescence intensity (MFI) value at 8,304. Both T and B cell crossmatches were strongly positive using the current serum, which indicated a significant shift in the patient's antibody reactivity within just seven days. Notably there were no Class I DSA to the first KP donor, and Class II antibody testing remained negative. We suspected that the positive antibody and FCXM results were likely attributed to thymoglobulin interference rather than an immune response. Published studies demonstrate that thymoglobulin can influence the results of the solid-phase antibody assay. Biological binding to T cells potentially engages with the anti-human IgG, resulting in a positive flow crossmatch. We recommended repeating antibody testing in a few weeks once the effects of thymoglobulin would have likely dissipated. Indeed, the most recent serum from 4/8/24 revealed only a few HLA-B specificities with low MFI values, indicating the interfering effect has decreased and the antibody results were once more clearly interpretable. (Fig1).
Conclusion: This case highlights the potential interference of thymoglobulin with crucial and complicated HLA laboratory tests. Sera containing thymoglobulin may induce false positive reactivity in both bead assays and flow cytometric crossmatching. Hence, it's essential to always consider the impact of a patient’s recent therapies on laboratory testing when unexpected results are seen.