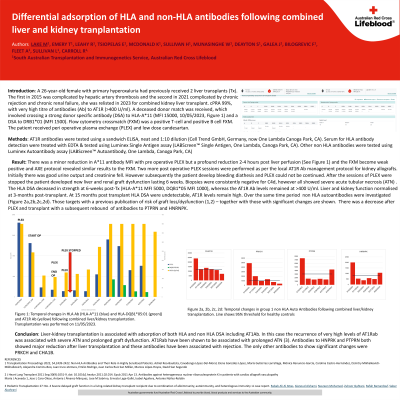
Body: A 26-year-old female with a history of primary hyperoxaluria had previously received 2 liver transplants (Tx). The first in 2015 was complicated by hepatic artery thrombosis and the second in 2021 complicated by chronic rejection and chronic renal failure and she was relisted in 2023 for combined kidney liver transplant. She was highly sensitized with cPRA of 98.8%, with very high titre of antibodies (Ab) to AT1R (>400 U/ml). A deceased donor match was received, which involved crossing a strong donor specific antibody (DSA) to HLA-A*11 (MFI 15000, 10/05/2023, Figure 1) and a DSA to DRB1*01 (MFI 1500). The flow cytometry crossmatch (FXM) using pre transplant sera indicated a positive T-cell and positive B cell FXM using neat and 1/8 diluted sera. The offer was accepted, with the liver transplant proceeding 6 hours prior to the kidney transplant. The patient received postoperative plasma exchange (PLEX) and low dose candesartan, and the HLA DSA and AT1R Ab were monitored.
The liver adsorbed the HLA-A*11 DSA by 1-hour post-Tx, (11/05/2023 13:30, Figure 1) and a marked reduction in MFI was observed prior to commencement of PLEX, returning a weak positive T-cell, but negative B-cell FXM (T-cell FXM was negative at 1/8 dilution). The HLA-A*11 DSA increased to moderate levels 2-weeks post-Tx (MFI ~4000), and strong at 3 weeks post-Tx (MFI ~11000) and included de novo HLA DSA to DQB1*05 (MFI ~3000). Over the same time, AT1R Ab was only partially adsorbed, dropping from >400U/ml to ~100U/ml. Moreover, the AT1R Ab were rapid to rebound to >250 U/ml 2 weeks post-transplant and returning to >400 U/ml 3 weeks post-transplant. Due to patient instability PLEX could not be continued and there was prolonged liver and renal graft dysfunction lasting 6 weeks. Biopsies were consistently negative for C4d.
Interestingly, the HLA DSA deceased in strength at 6-weeks post-Tx (HLA-A*11 MFI 5000, DQB1*05 MFI 1000), whereas the AT1R Ab levels remained at >400 U/ml. However, liver and kidney function had normalised at 3-months post-transplant and remained so at 12 months post-transplant.
Conclusion: Liver-kidney transplantation in the presence of strong HLA DSA and high titre AT1R Ab was associated with prolonged graft dysfunction of liver and kidney lasting 6 weeks. HLA DSA was more highly adsorbed by the liver compared to AT1R Ab.