Aim: Antibodies directed against the HLA antigens of a transplanted organ are associated with a risk for rejection and can be detected using the crossmatch assay as well as HLA antibody detection panels. Multiple studies established correlations between flow cytometric crossmatch (FCXM) and transplant outcomes; therefore, consistent inter-laboratory FCXM results are critical for successful and safe organ transplantation. We aimed to evaluate the degree and nature of inter-laboratory FCXM variability by analyzing ASHI Proficiency Testing (PT) antibody and crossmatching (AC) survey results between 2018 and 2023.
Method: FCXM and antibody specificity data were extracted from the ASHI Proficiency Testing Data Center. FCXM results were graded based on 80% consensus among participating laboratories. Results that did not agree with consensus were graded Discrepant. Results that did not reach consensus were not graded (NG1 score). Individual antibody specificities were graded based on 90% consensus.
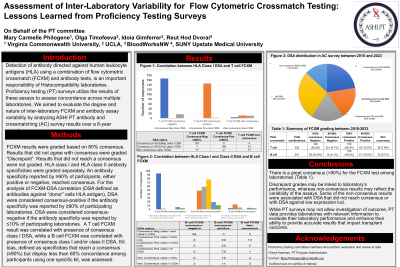
Results: National and international laboratories representing 22 countries produced >10,000 individual T cell and B cell FCXM results. Of the 360 T cell and 350 B cell FCXM combinations, 92.5% T cell and 91.7% B cell crossmatches reached consensus across 147 to 159 laboratories (Table 1). T cell FCXM that reached positive or negative consensus correlated with the presence or absence of Class I donor specific HLA antibodies (DSA), respectively. B cell FCXM that reached positive or negative consensus correlated with the presence or absence of Class I and/or Class II DSA, respectively. Only 7.9% of T cell and 9.7% of B cell FCXM combinations, did not reach consensus and received NG1 score. As expected, NG1 results were associated with DSA that did not reach consensus.
Conclusion: Discrepant grades for FCXM results that reached consensus may be linked to laboratory performance, whereas lack of consensus may reflect the variability of the assays and the presence of low level DSA. Our analysis shows that despite differences in testing protocols, the consensus for a FXCM test can be achieved in over 90% of cases. This is important since although transplant centers may vary in the levels of immunological risk they are willing to accept, it is critical that the analytical assessment is performed in a comparable manner across laboratories.