Aim: To understand the merits of high-resolution HLA-typing, we set to evaluate the impact of human leukocyte antigen (HLA) mismatches at the eplet level, on the risk of acute rejection and graft failure in heart transplants. Additionally, we also sought to determine whether eplet matching provides predictive advantages over low-resolution antigen matching.
Method: We conducted high-resolution next-generation sequencing HLA-typing on 200 donor-recipient pairs to identify Class I (HLA-A, -B, and -C) and Class II (HLA-DR, -DP, and -DQ) mismatches. Heart biopsies were periodically collected and graded for acute cellular rejection from grade 0R (no rejection) to 3R (severe rejection). We employed generalized linear mixed modeling to explore the associations between eplet mismatches and rejection gradings, adjusting for clinical variables such as the ages and sexes of donors and recipients, as well as donor and recipient BMI. Additionally, a survival analysis was conducted to elucidate the impact of eplets on graft failure. We compared AIC prediction error values between the eplet and antigen models to establish which was more effective in predicting poor outcomes.
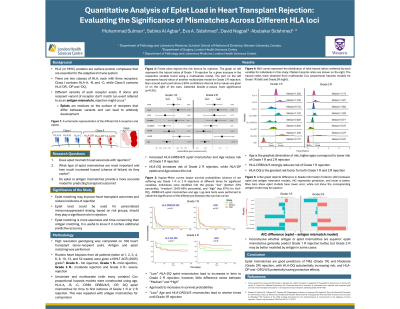
Results: Analysis indicates that mismatches in HLA-DQ are particularly associated with an increased risk of mild (Grade 1R) and moderate (Grade 2R) rejection (p < 0.05). HLA-DRB3/4/5 confers a protective effect against mild rejection, increasing the time to first incidence and the number of occurrences (p < 0.05). No significant correlation between eplet load and graft failure were found. Eplet mismatch models did not consistently have lower prediction error, as compared to their antigen mismatch counterparts (Fig-1-a and-b).
Conclusion: HLA-typing offers benefits in minimizing cases of heart transplant rejection; however, the benefits of high-resolution typing remain unclear. HLA-DQ mismatch significantly increases the risk and number of instances of rejection. Knowledge of donor-recipient HLA mismatches can be used for creating accurate personalized immunosuppressant dosing regimens.