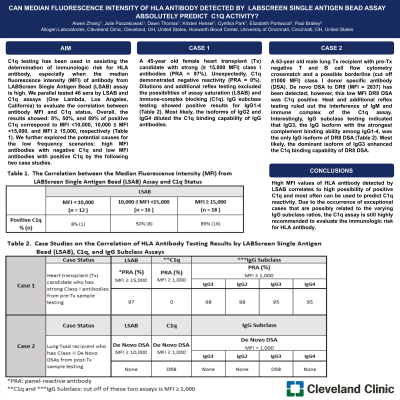
Body: C1q testing has been used in assisting the determination of immunologic risk for HLA antibody, especially when the median fluorescence intensity (MFI) of antibody from LABScreen Single Antigen Bead (LSAB) assay is high. We parallel tested 46 sera by LSAB and C1q assays (One Lambda, Los Angeles, California) to evaluate the correlation between antibody MFI and C1q status. Overall, the results showed: 8%, 50%, and 89% of positive C1q correspond to MFI <10,000, 10,000 ≤ MFI <15,000, and MFI ≥ 15,000, respectively (Table 1). We further explored the potential causes for the low frequency scenarios: high MFI antibodies with negative C1q and low MFI antibodies with positive C1q by the following two case studies. CASE 1: A 45-year old female heart transplant (Tx) candidate with strong (≥ 15,000 MFI) class I antibodies (PRA = 97%). Unexpectedly, C1q demonstrated negative reactivity (PRA = 0%). Dilutions and additional reflex testing excluded the possibilities of assay saturation (LSAB) and immune-complex blocking (C1q). IgG subclass testing showed positive results for IgG1-4 (Table 2). Most likely, the isoforms of IgG2 and IgG4 diluted the C1q binding capability of IgG antibodies. CASE 2: A 63-year old male lung Tx recipient with pre-Tx negative T and B cell flow cytometry crossmatch and a possible borderline (Cut off ≥1000 MFI) class I donor specific antibody (DSA). De novo DSA to DR8 (MFI = 2837) has been detected; however, this low MFI DR8 DSA was C1q positive. Heat and additional reflex testing ruled out the interference of IgM and immune complex of the C1q assay. Interestingly, IgG subclass testing indicated that IgG3, the IgG isoform with the strongest complement binding ability among IgG1-4, was the only IgG isoform of DR8 DSA (Table 2). Most likely, the dominant isoform of IgG3 enhanced the C1q binding capability of DR8 DSA.
Conclusion: High MFI values of HLA antibody detected by LSAB correlates to high possibility of positive C1q and most often can be used to predict C1q reactivity. Due to the occurrence of exceptional cases that are possibly related to the varying IgG subclass ratios, the C1q assay is still highly recommended to evaluate the immunologic risk for HLA antibody.