(P121) Use of intermediate-resolution deceased donor molecular typing in organ allocation systems could increase the fraction of HLA-compatible donor offers
Aim: Rapid deceased donor HLA typing by sequence-specific oligonucleotide (SSO) methods are reported to kidney allocation systems and outcomes registries at a low-resolution antigen level, which results in a loss of information. We aimed to measure the potential utility of capturing intermediate-resolution HLA genotype lists instead of antigen-level typing for determining organ offers in allocation systems.
Method: We sampled 800 9-locus two-field genotypes each from 6 different US populations using the HLA genotype frequency distribution from the OPTN CPRA panel. To simulate typing ambiguity from each sampled input HLA single-locus genotype, we developed an Allele Ambiguity Utility program for the Werfen LIFECODES® Rapid sequence-specific oligonucleotide (SSO) kit, which outputs a list of possible full-field HLA genotypes. Ambiguous HLA genotype lists were compressed to two-field antigen recognition domain (ARD) level and high resolution genotype probabilities imputed using HLA haplotype frequencies from NMDP. Imputation prediction performance was measured using calibration plots and statistics.
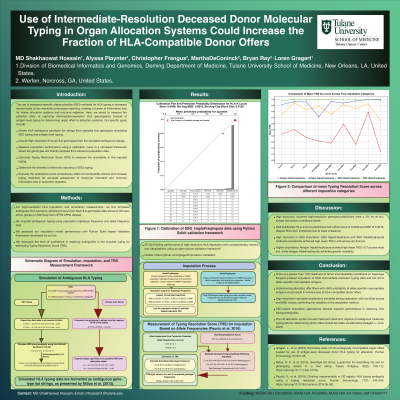
Results: For single-locus genotype predictions, the fraction of most probable high resolution assignments that were incorrect was no greater than 2% for any locus for higher probability predictions outside of the bottom lowest-confidence decile. We provide an example calibration plot for HLA-A locus genotype predictions across the entire dataset (Figure 1). High resolution imputation predictions based on intermediate resolution typing were very well-calibrated, with low Brier scores and bin-average measured-squared error (MSE) distances (Brier score 0.0496 of individual-level predictions and MSE 0.0016 for deciles based on most probable HLA-A high resolution genotypes). Receiver Operating Characteristic (ROC) Area Under the Curve statistics were not useful indicators of imputation performance due to class imbalance, as nearly all predictions had high probability.
Conclusion: If allocation offer filters were implemented where transplant centers could choose to screen out organ offers that had ambiguous HLA typing but greater than 90% probability that any allele-specific unacceptable antigen were present in the donor, transplant candidates would miss out on very few potentially HLA-compatible donor offers.